
Introduction
Perimenopause rarely begins with a single dramatic event.
For many women, the first changes appear gradually, often years before their final menstrual period. Sleep becomes lighter. Stress feels harder to manage. Menstrual cycles become less predictable. PMS worsens. Mood shifts seem to appear without explanation.
At first glance, these changes can seem unrelated. They are often attributed to stress, ageing, or simply having a busy life. Yet beneath the surface, they may share a common biological thread.
One of the earliest hormonal changes during perimenopause is often a gradual decline in progesterone.
Although progesterone is best known for its role in reproduction and pregnancy, its influence extends far beyond fertility. It helps regulate sleep, supports the body’s response to stress, influences mood, contributes to bone health, and plays an important role in maintaining hormonal balance throughout the menstrual cycle.
Even more importantly, progesterone offers a valuable window into understanding the early stages of perimenopause. Rather than acting in isolation, progesterone functions within an intricate network of interconnected physiological systems. Communication among the brain, ovaries, nervous system, thyroid, metabolism, gut, liver, and the body’s circadian biology all influences how progesterone is produced, utilised, and regulated.
This systems-based perspective helps explain why two women with similar hormone levels can experience very different symptoms, and why addressing hormone health often requires looking beyond hormones alone.
The body is constantly adapting to changes occurring within and around it. Long before major hormonal shifts become obvious, those adaptations often begin communicating through subtle changes in sleep, mood, menstrual cycles, energy, and resilience to stress. These symptoms are not simply inconveniences to suppress. They are often important physiological signals that deserve to be understood within the broader context of the body’s remarkable ability to adapt.
Understanding progesterone is therefore about much more than understanding one hormone. It is about understanding one of the earliest biological changes of perimenopause and appreciating how the body’s interconnected systems work together throughout this important life transition.
To better understand how progesterone interacts with estrogen and testosterone during the menopause transition, read our guide Understanding Estrogen, Progesterone and Testosterone During Perimenopause and Menopause.
What Is Progesterone?
Most women have heard of estrogen. Far fewer realise that progesterone often provides some of the earliest clues that the menopause transition has begun.
For many women, progesterone begins changing several years before menopause itself. As its production becomes less consistent, symptoms such as disturbed sleep, anxiety, heavier periods, worsening PMS, and mood changes may begin to appear, even while menstrual periods remain regular.
This is one reason progesterone deserves far more attention than it often receives.
Although progesterone is best known for its role in fertility and pregnancy, it’s effects extend throughout the body. It functions as a whole-body signalling molecule, helping coordinate communication between multiple body systems.
Its receptors are found not only in the reproductive organs, but also throughout the brain, nervous system, bones, breasts, cardiovascular system, and other tissues. This widespread distribution helps explain why changing progesterone levels can influence so many aspects of health and wellbeing.
Rather than acting in isolation, progesterone works together with estrogen, testosterone, cortisol, melatonin, thyroid hormones, insulin, and many other chemical messengers. Together, these hormones help regulate sleep, metabolism, stress resilience, reproduction, tissue repair, and healthy ageing.
Like all hormones, progesterone does not simply provide a chemical signal. It forms part of an intricate communication network that allows the body to continuously adapt to changing circumstances while maintaining internal balance, a process known as homeostasis.
What Does Progesterone Do?
One reason progesterone is so important is that its influence extends well beyond reproduction. Among its many functions, progesterone helps:
- Support healthy ovulation and menstrual cycles
- Prepare the uterus for pregnancy
- Help regulate the uterine lining
- Balance many of estrogen’s effects
- Support healthy breast tissue
- Maintain bone health
- Help regulate the nervous system
- Support stress resilience
- Promote restorative sleep by interacting with calming pathways in the brain
- Contribute to mood stability and emotional wellbeing
For decades, progesterone rises and falls in a carefully coordinated monthly rhythm alongside estrogen. These fluctuations are not random. They provide important biological signals that help coordinate reproductive function while also influencing sleep, metabolism, immune function, tissue repair, and many other physiological processes.
From a systems perspective, progesterone is therefore not simply a fertility hormone. It is one of the body’s key biological messengers, helping multiple systems communicate, adapt, and function in harmony.
Many women tell me they had never heard much about progesterone until they began experiencing sleep problems, anxiety, or heavier periods in their forties.
In clinical practice, these are often some of the earliest clues that hormone patterns are beginning to change.
Because menstrual periods may still be occurring regularly, many women are reassured that their hormones are “normal”. In reality, progesterone production can begin declining years before menopause, even while cycles continue.
Recognising these early changes may help explain why symptoms often appear long before menopause itself.
Where Is Progesterone Produced?
Before menopause, progesterone is produced primarily by the corpus luteum, a temporary hormone-producing structure that forms in the ovary after ovulation.
Each month after ovulation, the emptied follicle transforms into the corpus luteum. Rather than being left over, this remarkable structure has a new purpose: producing progesterone during the second half of the menstrual cycle.
If pregnancy does not occur, the corpus luteum naturally breaks down after around two weeks. Progesterone levels fall, the uterine lining is shed, and a new cycle begins.
If pregnancy does occur, the corpus luteum continues producing progesterone until the placenta gradually takes over hormone production.
Although the ovaries produce most progesterone during the reproductive years, they are not working alone. Smaller amounts are also produced by the adrenal glands and, in very small quantities, by the brain and other tissues. This reflects an important principle seen throughout human physiology: the body often uses multiple organs and tissues to support essential biological functions rather than relying on a single source.
After menopause, ovulation no longer occurs, meaning the corpus luteum is no longer formed. As a result, ovarian progesterone production falls dramatically. Small amounts continue to be produced by the adrenal glands and some other tissues, but these levels are considerably lower than during the reproductive years.
Many women are surprised to learn that progesterone is produced only after ovulation.
This means that having a monthly period does not necessarily mean progesterone production is optimal.
As ovulation becomes less consistent during perimenopause, progesterone production may begin declining while menstrual cycles continue, helping explain why symptoms often appear years before menopause itself.
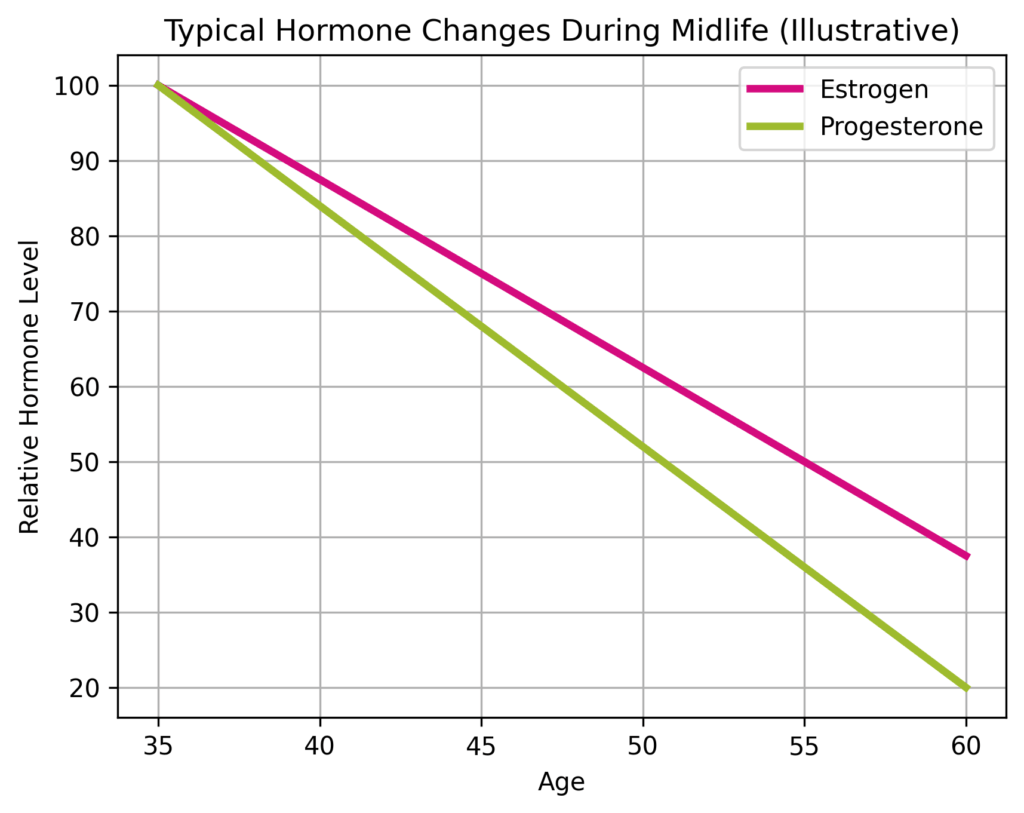
Why Does Progesterone Decline Before Estrogen?
One of the most common questions women ask is:
“If estrogen causes so many menopause symptoms, why are sleep problems, anxiety, heavier periods and worsening PMS often the first signs that something is changing?”
The answer lies in one simple but often overlooked biological fact. Progesterone can only be produced after ovulation.
No ovulation
No corpus luteum
No significant progesterone
Estrogen behaves differently. Unlike progesterone, estrogen continues to be produced throughout much of the menstrual cycle. Even as women enter perimenopause, estrogen production often continues, although it becomes increasingly unpredictable. Some months levels may be high, while in others they fall sharply.
By contrast, progesterone has a much narrower window of production. If ovulation is delayed, weaker than usual, or does not occur at all, progesterone production falls immediately.
This is why progesterone often provides one of the earliest physiological signals that the menopause transition has begun.
Perimenopause Is Often a Story of Changing Ovulation
One of the biggest misconceptions about perimenopause is that hormones simply begin declining together.
In reality, the earliest change is often that ovulation becomes less reliable. Some months, an egg is released normally. Some months ovulation is delayed. Some months it may not occur at all. These are known as anovulatory cycles.
Importantly, many women continue having apparently regular menstrual periods during this time. From the outside, everything appears normal. Inside the body, however, hormone patterns are already changing.
Without regular ovulation, progesterone production becomes increasingly inconsistent. Estrogen may still be present, but its long-term biological partner is no longer being produced in the same coordinated rhythm.
From a systems perspective, this is not simply a decline in one hormone. It represents a gradual loss of the beautifully coordinated communication that has synchronised multiple body systems for decades.
Progesterone is only one part of the complex hormonal changes that occur during the menopause transition. For a broader overview of what happens during each stage and the common symptoms women may experience, explore our Menopause Knowledge Hub.
Why Symptoms Can Appear Years Before Menopause
This helps explain one of the greatest sources of confusion for many women.
“I’m still having regular periods. Why do I suddenly have anxiety, poor sleep, heavier periods and feel completely different?”
Because menstrual bleeding does not necessarily tell us whether healthy ovulation has occurred. A woman may continue bleeding every month while producing significantly less progesterone during the second half of her cycle.
Menstrual bleeding is still occurring. The underlying hormonal pattern has already changed. In many cases, this shift begins several years before menopause itself.
Could Low Progesterone Explain Your Symptoms?
One of the reasons progesterone receives far less attention than it deserves is that its decline can affect many different body systems.
For some women, the first signs are subtle. Others experience several changes over a relatively short period. Because these symptoms often develop gradually, they are frequently attributed to ageing, stress, or simply having a busy life.
While no single symptom confirms low progesterone, recognising common patterns can help explain why many women begin feeling “different” years before menopause itself.
Sleep Changes
Sleep disruption is often one of the earliest and most common symptoms women notice.
Many women find themselves waking around 2 or 3 a.m., struggling to fall back asleep, or waking feeling unrefreshed despite spending enough time in bed.
Progesterone interacts with some of the brain’s natural calming pathways and helps support deep, restorative sleep (GABA pathway). As progesterone production becomes less consistent, sleep is often one of the first systems to notice the change.
Since progesterone has important effects on sleep quality, you may also be interested in our Sleep & Circadian Rhythm Knowledge Hub, where we explore the science of restorative sleep and practical strategies for improving it.
Anxiety and Feeling More “On Edge”
Many women describe a new sense of nervousness or emotional sensitivity during their forties.
Situations that once felt manageable suddenly feel overwhelming. Small problems seem larger, patience becomes shorter, and everyday stress feels harder to recover from.
This is not simply about willpower or coping better. Progesterone helps support the nervous system, and changing hormone patterns may contribute to feeling less resilient during times of stress.
Heavier or Longer Periods
Progesterone helps regulate the growth of the uterine lining after ovulation.
When progesterone production declines while estrogen continues stimulating the lining, menstrual bleeding may become heavier, last longer, or become less predictable than it was previously.
For many women, this is one of the earliest physical signs that hormone patterns are beginning to change.
Worsening PMS
Women often tell me: “I’ve always had a little PMS, but this feels completely different.”
Mood swings, breast tenderness, bloating, headaches, irritability, food cravings, and emotional sensitivity may become more noticeable during the second half of the menstrual cycle as progesterone becomes less consistent.
Reduced Stress Resilience
One of the most difficult symptoms to describe is simply not feeling like yourself.
Many women say they become more reactive, less patient, and more easily overwhelmed than they used to be. Challenges that once felt manageable now require considerably more emotional energy.
Because progesterone interacts closely with the nervous system, sleep, and stress physiology, declining levels may influence how resilient we feel during periods of physical or emotional stress.
Mood Changes
Hormones influence many of the chemical messengers involved in mood regulation.
As progesterone begins fluctuating, some women notice increased irritability, tearfulness, low mood, or a greater sense of emotional vulnerability. These changes are often most noticeable during the second half of the menstrual cycle, when progesterone would normally be at its highest.
Every Woman’s Experience Is Different
Not every woman experiences the same symptoms, nor are changing hormone patterns the only factor involved.
Sleep quality, circadian biology, stress physiology, thyroid function, metabolic health, nutritional status, gut health, and overall lifestyle all influence how hormonal changes are experienced.
This helps explain why two women with similar progesterone levels may have very different symptoms and why supporting hormone health often requires looking beyond hormones alone.
Quick Recap: Key Signs of Declining Progesterone
- Sleep becomes lighter or more fragmented
- Anxiety or nervous system sensitivity increases
- Periods may become heavier or longer
- PMS becomes more noticeable
- Stress feels harder to manage
- Mood becomes less predictable
- Symptoms often begin while menstrual cycles are still regular
When Is Low Progesterone Normal?
Progesterone levels naturally change throughout a woman’s life.
Unlike many health conditions where lower hormone levels always indicate a problem, progesterone follows predictable biological patterns that reflect different stages of life. Understanding these patterns can help distinguish normal hormonal transitions from situations that may benefit from further investigation.
During Puberty
In the first few years after menstruation begins, ovulation is often irregular.
Without regular ovulation, progesterone production is naturally inconsistent while the brain, ovaries, and reproductive system establish the hormonal rhythms that will support the menstrual cycle throughout the reproductive years.
This is a normal part of development.
During Pregnancy
Progesterone rises dramatically during pregnancy.
Initially, it is produced by the corpus luteum. As pregnancy progresses, the placenta becomes the primary source of progesterone, producing levels far higher than those seen during the menstrual cycle.
These elevated levels help maintain pregnancy and support the developing baby.
During Breastfeeding
While breastfeeding, particularly during exclusive breastfeeding, ovulation may be delayed or temporarily suppressed. As a result, progesterone production remains lower until regular ovulation returns.
This is another normal physiological adaptation that allows the body to prioritise infant care and recovery after pregnancy.
During Perimenopause
Perimenopause is the most common time for progesterone levels to become less consistent.
As ovulation becomes increasingly irregular, progesterone production fluctuates from cycle to cycle. Some months levels may be close to normal, while in others very little progesterone is produced. This changing pattern often explains why symptoms seem unpredictable and why many women feel well one month but struggle the next.
After Menopause
Following menopause, the ovaries no longer release eggs and regular ovulation ceases. Without ovulation, the ovaries no longer produce significant amounts of progesterone.
Small amounts continue to be produced by the adrenal glands and some other tissues, but levels remain much lower than during the reproductive years. This is a normal physiological adaptation to a new stage of life with different hormonal priorities.
After Stopping Hormonal Contraception
Hormonal contraceptives work primarily by preventing ovulation.
Because progesterone is produced after ovulation, the body produces very little of its own progesterone while using most combined oral contraceptives. After stopping the pill, natural ovulation does not always return immediately. For some women, regular cycles resume within weeks, while for others the communication between the brain and ovaries takes longer to re-establish.
During this transition, progesterone production may remain lower until consistent ovulation returns.
For most women, this is a temporary physiological adaptation rather than a sign that something has gone wrong. However, if menstrual cycles do not return after several months, or symptoms persist, further assessment may be appropriate to identify any underlying factors that could be delaying recovery.
As this process unfolds, the body is re-establishing its own hormonal rhythms, including the coordinated communication between the brain, ovaries, and circadian biology that supports healthy ovulation.
When Should Low Progesterone Be Investigated?
Although lower progesterone is expected during certain stages of life, low levels outside these situations may sometimes indicate that ovulation is not occurring regularly. Possible contributing factors include:
- Polycystic ovary syndrome (PCOS)
- Functional hypothalamic amenorrhoea
- Premature ovarian insufficiency
- Thyroid dysfunction
- Hyperprolactinaemia
- Chronic stress
- Very low energy intake or excessive exercise
- Certain medications
- Hormonal contraception that suppresses ovulation
The goal is not simply to increase progesterone levels, but to understand why ovulation has changed in the first place. In many cases, addressing the underlying cause allows healthier hormonal rhythms to return.
One of the most common misunderstandings I encounter in practice is the belief that regular menstrual bleeding always means normal progesterone production.
In reality, progesterone depends on ovulation, not on bleeding itself.
A woman can continue having apparently regular periods while ovulating less consistently and producing significantly less progesterone during the second half of her cycle.
Understanding this simple distinction often explains why symptoms can begin several years before menopause is officially reached.
Quick Recap: When Is Low Progesterone Normal?
- Puberty, while menstrual cycles are maturing
- Pregnancy, when progesterone rises dramatically
- Breastfeeding, while ovulation is temporarily suppressed
- Perimenopause, as ovulation becomes less consistent
- Menopause, when regular ovulation has ceased
- After stopping hormonal contraception (the pill), as it suppresses ovulation
- Outside these situations, persistently low progesterone may warrant further assessment, particularly if accompanied by symptoms such as PMS, irregular menstrual cycles, or other symptoms of hormone change.
Although changes in progesterone are a normal part of perimenopause, symptoms such as very heavy or prolonged bleeding, bleeding after menopause, persistent pelvic pain, or rapidly worsening symptoms should always be assessed by your healthcare provider to exclude other medical conditions.
What Can Contribute to Low Progesterone?
One of the biggest misconceptions about progesterone is that it declines for a single reason.
In reality, progesterone production reflects the function of an entire physiological network. Because progesterone is produced after ovulation, anything that affects communication between the brain, ovaries, adrenal glands, thyroid, metabolism, digestive system, or the body’s overall energy balance may influence progesterone production.
Rather than asking, “What caused my progesterone to become low?”, a more helpful question is:
“Which body systems may be influencing my ability to ovulate consistently?”
This systems-based perspective often provides a more complete understanding of hormone health than focusing on progesterone alone.
1. Perimenopause: The First Hormonal Transition
For most women, the earliest and most common reason for declining progesterone is perimenopause.
As ovarian function gradually changes, ovulation becomes less predictable. Some cycles still release an egg and produce healthy amounts of progesterone, while others do not. This explains why symptoms often appear intermittently during the early stages of perimenopause and why one month can feel completely different from the next.
Importantly, these changes often begin while menstrual periods are still occurring regularly.
Rather than representing ovarian failure, these changes reflect the body’s gradual adaptation as it transitions from the reproductive years towards menopause.
2. Circadian Biology and Poor Sleep
Healthy progesterone production begins long before ovulation. It depends on the smooth coordination of the brain, nervous system, endocrine system and ovaries, all of which are strongly influenced by circadian biology.
The body’s master clock in the brain uses natural morning light to synchronise hundreds of biological processes, including hormone signalling, sleep-wake cycles, metabolism and reproductive function. Throughout the day, this internal timing system helps coordinate the hormonal communication required for healthy ovulation.
When circadian rhythms are disrupted by insufficient morning light, excessive evening artificial light, shift work, irregular sleep schedules, or chronic sleep deprivation, this finely tuned communication may become less efficient.
Because hormone production is closely linked with the body’s internal timing system, optimising circadian biology may support overall hormone health. Learn more in our Circadian Health Pillar.
Research increasingly suggests that circadian disruption may influence reproductive hormone signalling, menstrual regularity and ovulation. While the relationship is complex and continues to be investigated, it reinforces an important principle:
Hormone health depends not only on what the body produces, but also on when those hormonal signals occur.
This is one reason why supporting circadian biology through regular sleep patterns and morning daylight exposure may benefit healthy hormone regulation far beyond menopause alone.
One of the most fascinating discoveries is how the body’s circadian biology influences hormone production, metabolism, sleep, and healthy ageing. We explore these connections in depth in our Melatonin, Sunlight, Sleep and Hormones guide.
3. Chronic Stress and Nervous System Adaptation
Stress is often blamed for hormonal problems, but the relationship is more sophisticated than many people realise. When the body experiences prolonged physical or emotional stress, its primary priority becomes survival rather than reproduction.
The brain continuously assesses internal and external conditions before deciding whether reproduction is a good biological investment. If it perceives ongoing stress, illness, inflammation or insufficient resources, reproductive hormone signalling may become less consistent.
Over time, chronic activation of the stress response can influence communication between the hypothalamus, pituitary gland and ovaries, making ovulation less reliable and progesterone production more variable.
This does not mean that stress “uses up” progesterone. Rather, it reflects the body’s remarkable ability to prioritise immediate survival while temporarily reducing investment in reproductive function until conditions improve.
Chronic stress can influence ovulation, cortisol regulation, and progesterone production. Learn more about these interconnected pathways in our upcoming guide to Stress, Cortisol and Hormone Health. In the meantime, explore our collection of stress, cortisol and adrenal fatigue articles.
4. Gut Health
The digestive system may not seem like an obvious place to look when discussing progesterone, yet healthy hormone production depends on healthy gut function.
The gut supports healthy hormone regulation in several important ways.
It enables the absorption of nutrients needed for hormone production, helps regulate inflammation, communicates continuously with the brain through the gut-brain axis, supports immune function and influences the metabolism of hormones such as estrogen through the estrobolome.
Poor digestive health, persistent inflammation, altered gut microbial balance, or impaired nutrient absorption may influence the broader physiological environment required for healthy hormone production.
Rather than acting independently, the gut forms part of an interconnected communication network linking the digestive system, nervous system, immune system and endocrine system.
Gut health plays an important role in hormone regulation, nutrient absorption, and inflammation. We’ll explore these connections further in our Gut Health and Microbiome guide and our comprehensive collection of Gut and digestive health guides, articles and downloads in the Gut Health and Microbiome Knowledge Hub.
5. Blood Sugar Regulation and Metabolic Health
Maintaining stable blood sugar is important for far more than diabetes prevention.
The body constantly monitors energy availability before committing resources to reproduction. Large fluctuations in blood glucose, insulin resistance and impaired metabolic health may all influence the hormonal signals that support regular ovulation.
Healthy metabolism provides the energy required for hormone production, tissue repair, and reproduction. When metabolic function becomes impaired, the body may shift its priorities towards maintaining essential functions before supporting reproductive processes.
This is one reason why improving metabolic health often supports healthy hormone regulation at the same time.
Metabolic health also influences hormone regulation. Discover how blood sugar balance, insulin sensitivity, and energy metabolism interact with hormonal health in our Metabolic Health Pillar.
6. Thyroid Function
The thyroid gland influences virtually every cell in the body, including the reproductive system.
Thyroid hormones help regulate metabolism, energy production and the communication between the brain and ovaries that supports regular ovulation. When thyroid function becomes impaired, menstrual cycles may change, ovulation may become less predictable and progesterone production may decline as a consequence.
For this reason, thyroid function should always be considered when investigating persistent hormonal symptoms, particularly if fatigue, cold intolerance, constipation, hair loss or unexplained weight changes are also present.
Because thyroid function and reproductive hormones often influence one another, we’ll explore these interactions in our upcoming guide to Thyroid Health and Hormones.
7. Nutritional Status
Hormones cannot be produced without adequate nutritional building blocks.
Healthy progesterone production depends on adequate energy intake together with sufficient vitamins, minerals, healthy fats, and protein. Particular nutrients that appear important for normal hormone production include zinc, magnesium, vitamin B6, vitamin D, selenium, iodine, iron and adequate dietary protein.
Low ferritin deserves particular attention. Iron deficiency may be present even when haemoglobin remains within the normal range and can contribute to fatigue, poor thyroid function and reduced resilience, all of which may indirectly influence reproductive health.
Nutrition alone rarely explains low progesterone, but inadequate nutrition can make it more difficult for the body to maintain healthy hormonal rhythms.
Nutrition provides many of the building blocks required for healthy hormone production. Our explores the dietary patterns, nutrients and lifestyle strategies that support healthy hormone and metabolic function. Explore our key nutrition guides and article in the Nutrition Knowledge Hub.
8. Low Energy Availability
The body continuously assesses whether enough energy is available to support reproduction safely.
Very restrictive diets, prolonged fasting, excessive exercise, eating disorders or chronic under-fuelling may all reduce the energy available for ovulation. This adaptive response is sometimes referred to as low energy availability and is increasingly recognised as an important cause of disrupted menstrual cycles in women of all ages.
From the body’s perspective, delaying reproduction during periods of insufficient energy is a protective survival mechanism rather than a malfunction.
9. Hormonal Contraception
Hormonal contraceptives primarily work by suppressing ovulation.
Because progesterone is naturally produced after ovulation, women taking combined oral contraceptives produce very little of their own progesterone during treatment. Instead, synthetic hormones provide contraception by altering the hormonal signals that normally regulate the menstrual cycle.
After stopping the pill, some women resume ovulation quickly, while for others it may take several months for normal hormonal rhythms to be restored.
Understanding this transition helps explain why hormone-related symptoms may temporarily appear after discontinuing hormonal contraception without necessarily indicating permanent hormonal dysfunction.
10. Other Medical Conditions
Several medical conditions may also contribute to reduced progesterone production by affecting ovulation or reproductive hormone signalling. These include:
- Polycystic ovary syndrome (PCOS)
- Functional hypothalamic amenorrhoea
- Premature ovarian insufficiency
- Thyroid disorders
- Hyperprolactinaemia
- Certain medications
- Chronic inflammatory conditions
These conditions require individual assessment, and progesterone should always be considered within the broader clinical picture rather than in isolation.
One of the most valuable shifts I see in clinical practice occurs when women stop asking, “How do I increase my progesterone?” and begin asking, “What does my body need in order to ovulate well?”
That small change in perspective often transforms the entire conversation.
Instead of chasing a single hormone, we begin supporting the systems that regulate it, including circadian biology, sleep, stress resilience, metabolic health, thyroid function, nutrition, gut health, and healthy ovarian communication.
Progesterone is rarely the starting point. More often, it is the messenger that tells us how well these systems are working together.
Quick Recap: What Can Contribute to Low Progesterone?
- Perimenopause and changing ovulation patterns
- Circadian rhythm and sleep,
- Chronic stress and altered brain-ovary communication
- Gut dysfunction and impaired nutrient absorption
- Blood sugar imbalance and metabolic dysfunction
- Thyroid disorders
- Nutritional deficiencies and low ferritin
- Low energy availability from restrictive eating or excessive exercise
- Hormonal contraception and recovery after stopping the pill
- Medical conditions that affect ovulation
Progesterone, Perimenopause and the Bigger Picture
One reason progesterone deserves more attention is that it often provides one of the earliest clues that the menopause transition has begun. Long before periods stop completely, many women begin noticing subtle but meaningful changes such as:
- Lighter, less restorative sleep
- Increased anxiety or feeling more easily overwhelmed
- Heavier or more irregular periods
- Worsening PMS
- Reduced resilience to stress
- Mood changes
- Breast tenderness
These symptoms are often dismissed as stress, ageing, or simply having a busy life. Sometimes those factors do play a role. They may also reflect changing progesterone patterns occurring beneath the surface as the body gradually transitions through perimenopause.
Understanding this shift can help women make sense of symptoms that otherwise seem disconnected or confusing. More importantly, it offers an opportunity to support health proactively rather than waiting until symptoms become overwhelming.
Perimenopause is not a sudden event that begins with the final menstrual period. It is a gradual biological transition during which the ovaries, brain, nervous system, metabolism, and other hormone-regulating systems continuously adapt to changing reproductive priorities.
Just as puberty represents a period of profound hormonal transformation at the beginning of the reproductive years, perimenopause marks another important stage of physiological adaptation.
Understanding progesterone is therefore about much more than understanding one hormone. It provides an early window into the remarkable changes taking place throughout the body during this transition.
Progesterone is only one part of the complex hormonal changes that occur during the menopause transition. For a broader overview of what happens during each stage and the common symptoms women may experience, explore our Menopause Knowledge Hub.
Progesterone Is Not an Isolated Hormone
One of the biggest misconceptions about hormone health is the idea that hormones operate independently from the rest of the body. In reality, progesterone is influenced by a complex network of interconnected physiological systems.
Healthy progesterone production depends on healthy communication between multiple systems, including:
- Consistent ovulation
- The hypothalamic-pituitary-ovarian (HPO) axis
- The nervous system and stress response
- Circadian biology and restorative sleep
- Metabolic health and insulin regulation
- Thyroid function
- Nutrient sufficiency
- Liver and gut health
This helps explain why two women with similar progesterone patterns may experience very different symptoms.
Hormones do not act alone. They operate within a larger physiological environment that influences how they are produced, metabolised, and used throughout the body. Rather than asking only:
“Is my progesterone low?”
a more helpful question is:
“What factors may be influencing my progesterone and overall hormone health?”
This systems-based perspective reflects one of the most important principles in modern physiology. The body is not a collection of isolated organs or hormones working independently. It is an intelligent, interconnected network that constantly communicates, adapts, compensates, and strives to maintain balance.
Progesterone is one part of that network.
Understanding how it interacts with the body’s broader physiological systems provides a stronger foundation for understanding perimenopause, making informed health decisions, and supporting long-term wellbeing. Visit our Hormone Health Pillar to explore evidence-informed guides on hormone balance, perimenopause, menopause, and healthy ageing.
The goal is not simply to restore one hormone. The goal is to support the biological systems that allow hormones to function in harmony. Read our comprehensive, 58-page practical guide to supporting progesterone: The Naturimedica Guide to Progesterone eBook.
Continue Your Progesterone Learning Journey
Progesterone is one of the most important hormones involved in women’s health, but understanding it requires more than simply learning what progesterone does. This guide is the first article in Naturimedica’s three-part Progesterone Knowledge Hub.
Part 1
Understanding Progesterone (this blog)
Learn why progesterone often begins changing years before menopause, how it influences sleep, mood, stress resilience, and hormone balance, and why it plays a much broader role than fertility alone.
Part 2
Progesterone Testing
Discover when progesterone testing is useful, the strengths and limitations of blood tests and DUTCH testing, why timing matters, and which other investigations, including thyroid function, iron status, insulin resistance, and nutrient deficiencies, can provide important clues.
Part 3
Supporting Healthy Progesterone Naturally
Explore the lifestyle, nutrition, circadian biology, stress management, gut health, movement, herbal medicine, and evidence-based supplement strategies that help support healthy progesterone production and the broader physiological systems that regulate hormone balance.
Together, these three guides provide a systems-based understanding of progesterone and its role in supporting healthy ageing during the menopause transition.
If you’re considering hormone therapy, understanding progesterone is an important first step. You may also find our HRT Decision Guide helpful for exploring the potential benefits, limitations, and questions to discuss with your healthcare practitioner.
Ready to Take the Next Step?
Understanding progesterone is an important first step. Applying that knowledge within the context of your own health is where it becomes truly valuable.
If you’re experiencing symptoms such as poor sleep, anxiety, heavier periods, worsening PMS, or other changes during perimenopause, the next article explains how progesterone can be assessed and why looking beyond a single hormone level often provides a more complete picture.
If you would like personalised support, you can also book a naturopathic consultation where we explore your symptoms using a systems-based approach that considers hormones alongside sleep, circadian biology, metabolism, gut health, nutrition, stress physiology, and healthy ageing.
👉 Please note that I consult with Australian-based clients only at present and I’m unable to assist individuals based elsewhere. I offer a free 20-minute initial discussion to review your circumstances and how I can help. Click on the link below to book.
Book Consultation Online
Learn about our wholistic approach to care in The Naturimedica Way and about Online Consultations.
I hope you found this guide informative, practical, and empowering, and that it has given you a clearer understanding of how supporting healthy progesterone function and overall hormone balance may positively influence sleep, energy, hormones, metabolism, and overall wellbeing.
I look forward to supporting you in achieving greater balance, energy and wellbeing.
Best of Health
Joanna Sochan
Wholistic Health and Lifestyle Therapist
Integrative health support combining clinical evidence, systems-based thinking and traditional naturopathic wisdom for lasting health and wellbeing
Evidence and Further Reading
Where applicable, content is informed by peer-reviewed research, clinical literature, and traditional naturopathic practice knowledge.
- PubMed: GABA System Modifications During Periods of Hormonal Flux Across the Female Lifespan
- PubMed: Mechanisms controlling the function and life span of the corpus luteum
- International Journal of Molecular Sciences: Key to Life: Physiological Role and Clinical Implications of Progesterone
- Austin Health Research Online: Efficacy of micronised progesterone for sleep: a systematic review and meta-analysis of randomised controlled trial data.
- America Society of Reproductive Medicine: Executive Summary of Stages of Reproductive Aging Workshop (STRAW+10)
- Endocrine Society: Review on reproductive ageing
Related Resources and Articles
- Menopause Symptoms and Systems Guide (eBook)
- Menopause Systems Self-Check (free download)
- Gut Health and Lifestyle
- The Gut-Brain connection explained
- Herbal Medicine Hub
Disclaimer: This content is for informational and educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making any changes to your health regimen, particularly if you are taking prescription or over-the-counter medications or have a medical condition.
Bio: Joanna Sochan is a Wholistic Natural Therapist and founder of Naturimedica Wholistic Wellcare. She has over 15 years of clinical experience working with complex health presentations, with a focus on gut health, food sensitivities, women’s hormone health (including perimenopause and menopause), metabolic health, weight regulation, and senior health. She works with clients Australia-wide and online, and also develops therapeutic programs, eCourses, and educational resources designed to support long-term, sustainable wellbeing. View full bio.

Leave A Comment